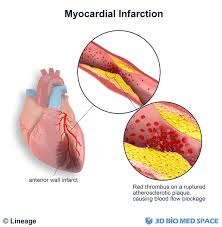
Myocardial infarction (Heart Attack):
It refers to localized area of cardiac necrosis due to ischemia. It affects man more than a women. Women are protected against MI during reproductive years, but postmenopausal hormone replacement therapy doesn’t protect women against MI.
Risk factors:
Aging, male gender, hypertension, smoking, DM, Hypercholesrolemia, Obesity, peripheral arterial disease, Family history.
Type of MI:
. Transmural infaction:
- . Most common type.
- . The artery is completely occlusive due to thrombus formation on disrupted plaque.
- . Involves the whole thickness of the myocardium.
- . All involves at least a portion of left ventricle.
- . New Q waves develop in an ECG.
- . ST segment elevation in ECG.
Subendocardial infaction:
- . In this case the artery supply the area is not completely occlusive, though there is disruption of plaques with thrombus formation.
- . Less common type.
- Involves the inner third of the myocardium.
- . Emcompasses the entire perfusion zone of the occluded artery.
- . Q waves are absent.
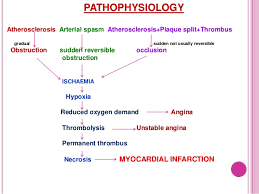
PATHOGENESIS Of MI (Heart Attack):
- Sudden disruption of atheromatous plaque.
- Subendocardial collagen and necrotic plaque contents are exposed.
- Platelets adhere to the exposed material and undergo aggregation , activation and released potent aggregates( thromboxane A2 & platelets factor 3 and 4 ).
- Platelets aggregation and release of mediators stimulate vasospasm.
- Within minutes the thrombus evolves to completely occluded the lumen of coronary vessels.
- Occlusion of the coronary vessels result in cessation of aerobic glycolysis and initiation of anaerobic glycolysis leading to:
- Inadequate production of ATP.
- Accumulation of toxic product ( lactic acid).
- The predominant mechanism of cell death is coagulation necrosis.
Biochemical changes:
- Anaerobic glycolysis = second.
- Loss of contractility = less than 2 min.
- ATP reduces to 50% of normal = 10 min.
- Irreversible cell injury = 20 – 40 min.
- Micro- vascular cell injury = more than 1 hour.
- Necrosis is complete = 6-12 hr.
Clinical features:
Chest pain;
- Sudden onset of severe retrosternal chest pain lasting more than 30 – 45 minutes.
- Pain is central and diffuse.
- Pain is tight, squeezing and choking in character.
- Pain is radiates to the left arm, jaw and neck.
- Pain is aggravated by exertion and emotion.
- Pain is not relived by nitroglycerine and rest.
Associated synptoms:
- Breathlessness
- Anxiety
- Diaphoresis
- Nausea and vomiting.
Cardiac enzyme in (Heart Attack):
| Elevated within | Peak | Return to normal | |
| CK-MB | 2-4 hr | 24hr | 72 hr |
| Troon in I & T | 2-4 hr | 28 hr | 7-10 days |
| LDH | 24 hr | 3-6 days | 8-14 days |
Microscopic Morphology of MI:
- Necrotic myocardium, acute inflammation ( 1- 3 days after MI ).
- Wave of macrophages that remove necrotic myocardium ( 5- 10 days after MI ).
- Formation of granulation tissue ( 1- 2 weeks after MI).
- Scaring ( most advanced by the end of 6th week ).
Localization of MI:
Distribution of coronary artery thrombosis;
- . Left anterior descending = 45%
- . Right coronary artery = 35%
- . Left circumflex coronary artery = 15%
- ECG consist of Q waves, ST segment elevation, T- waves inversion.
- Inverted T waves = area of ischemia at the periphery of the infarct.
- Elevated ST segment = injured myocardial cells surrounding the area os necrosis.
- New Q waves = area of coagulation necrosis.
- ECG diagnosis of MI can localized the affect site.
| Area of infarction | ECG changes | Artery involved |
| Inferior wall MI | II, III, a VF | Right coronary |
| Anteroseptal MI | V1-V2 | Left anterior descending |
| Anterolateral MI | V4-V6 | Left circumflex |
| Lateral wall MI | I,ALL, V5, V6 | Left circumflex |
| Posterior | V1-V4, ST segment, upright T waves | Posterior descending |
Complication of MI;
Arrhythmia:
. Heart rate less than 60.
. No cannon A waves.
Third degree heart block;
. Heart rate less than 60.
- Contractile dysfunction.
- Papillary muscle dysfunction.
- Right ventricular infarction.
- Myocardial rupture.
- Chamber dilation.
- Mural thrombus.
- Ventricular Aneurysm.
- Progressive late heart failure.
Treatment (DRUGS) Myocardial Infarction:
- Aspirin.
- Thrombolytics.
- Antiplatelet agents.
- Other blood-thinning medications.
- Pain relievers.
- Nitroglycerin.
- Beta blockers.
- ACE inhibitors.
Leave a Reply