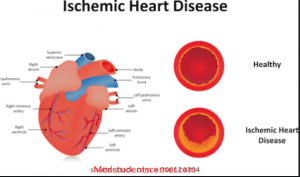
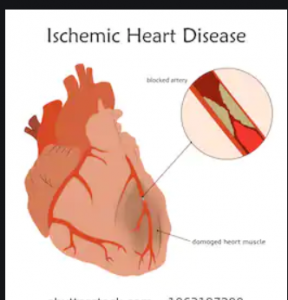
Ischemic heart disease:
It is a group of syndromes due to imbalance between myocardial oxygen demand and supply from the coronary arteries.It usually affect men of 45 years and up and female of 55 years and up.
Risk factors:
. Family history
. Tobacco
. Hypertension
. DM
. Lipid abnormalities.
. Increased LDL
. Decreased HDL.
Classification.
. Angina pectoral
. Chronic Ischemic heart disease
. Sudden cardiac death
. Myocardial inaction
Angina pectoris:
It refers to the transient cardiac ischemia without cell death resulting in substernal chest pain.
Types:
Stable Angina ( exertional Angina, classical Angina ).
It is also known as typical Angina and us the most common type.
. It is caused by coronary artery arthersclerosis characterized by
. Coronary artery stenosis is more than 75%.
. There is no plaque disruption and plaque associated thrombus.
RCG show ST segment depression due to subendocardial ischemia.
It is relieved by nitroglycerine and rest.
Prienzmetal variant Angina ( vasospactic Angina ).
It is episodic angina that occur at rest and is due to coronary artery spasm.
The attack of Prinzmetal angina are unrelated to physical activity, heart rate or blood pressure.
ECG show ST segment elevation due to transmural ischemia. Treatment is Nitroglycerine and calcium channel blockers.
Unstable Angina:
Also known as crescendo angina. It is characterized by bouts of chest pain at rest or minimal exertion. It is multi-vessel disease characterized by
. Coronary artery stenosis = variable.
. Plaque disruption = yes frequent
. Plaque associated thrombus = yes, not occlusive thrombus.
It is often the prodromeprodromal of subsequent acute MI. Unstable Angina , MI and sudden cardiac death are refers to as acute coronary syndromes.
Chronic Ischemic heart disease:
It refers to the cardiac finding in a patients who developed a progressive heart failure as a consequence of ischemic myocardial damage.
It is characterized by replacement of myocardial tissue with non- contractile scar tissue. It is diagnosed largely by the insidious onset of CHF in a patients who have had a past episodes of MI or anginal attacks.
Morphology:
. Enlarge and heavy heart.
. Left ventricular hypertrophy and dilation.
. Stenosing atherosclerosis of coronary artery.
. Myocardial hypertrophy.
. Subendocardial vacuolization.
. Scar of healed infarct.
Sudden cardiac death:
Unexpected death due to cardiac causes within 1 hour after onset of symptoms or without onset of symptoms.
The ultimate mechanism of sudden cardiac death is most often a lethal arrhythmia such as ventricular fibrillation. It is caused by;
. Congenital abnormalities.
. Aortic valve prolapse.
. Mittal valve prolapse.
. Myocarditis.
. Cardiomyopathy.
Pulmonary hypertension.
. Cardiac conduction system abnormalities.
Morphology:
. Market coronary atherosclerosis.
. Critical stenosis involving one or more of the three major vessels in 80 to 90%.
. Acute plaque disruption is common leading to thrombus formation and ultimately other complication.
. Healed myocardial inaction in about 40%
Subendocardial myocyte vacuolization.
Myocardial infaction:
It refers to localized area of cardiac necrosis due to ischemia. It affects man more than a women. Women are protected against MI during reproductive years, but postmenopausal hormone replacement therapy doesn’t protect women against MI.
Risk factors:
Aging, male gender, hypertension, smoking, DM, Hypercholesrolemia, Obesity, peripheral arterial disease, Family history.
Type of MI:
. Transmural infaction:
. Most common type.
. The artery is completely occlusive due to thrombus formation on disrupted plaque.
. Involves the whole thickness of the myocardium.
. All involves at least a portion of left ventricle.
. New Q waves develop in an ECG.
. ST segment elevation in ECG.
Subendocardial infaction:
. In this case the artery supply the area is not completely occlusive, though there is disruption of plaques with thrombus formation.
. Less common type.
Involves the inner third of the myocardium.
. Emcompasses the entire perfusion zone of the occluded artery.
. Q waves are absent.
PATHOGENESIS:
- Sudden disruption of atheromatous plaque.
- Subendocardial collagen and necrotic plaque contents are exposed.
- Platelets adhere to the exposed material and undergo aggregation , activation and released potent aggregates( thromboxane A2 & platelets factor 3 and 4 ).
- Platelets aggregation and release of mediators stimulate vasospasm.
- Within minutes the thrombus evolves to completely occluded the lumen of coronary vessels.
- Occlusion of the coronary vessels result in cessation of aerobic glycolysis and initiation of anaerobic glycolysis leading to:
- Inadequate production of ATP.
- Accumulation of toxic product ( lactic acid).
- The predominant mechanism of cell death is coagulation necrosis.
Biochemical changes:
- Anaerobic glycolysis = second.
- Loss of contractility = less than 2 min.
- ATP reduces to 50% of normal = 10 min.
- Irreversible cell injury = 20 – 40 min.
- Micro- vascular cell injury = more than 1 hour.
- Necrosis is complete = 6-12 hr.
Clinical features:
Chest pain;
- Sudden onset of severe retrosternal chest pain lasting more than 30 – 45 minutes.
- Pain is central and diffuse.
- Pain is tight, squeezing and choking in character.
- Pain is radiates to the left arm, jaw and neck.
- Pain is aggravated by exertion and emotion.
- Pain is not relived by nitroglycerine and rest.
Associated synptoms:
- Nausea and vomiting.
Cardiac enzyme:
| Elevated within | Peak | Return to normal | |
| CK-MB | 2-4 hr | 24hr | 72 hr |
| Troon in I & T | 2-4 hr | 28 hr | 7-10 days |
| LDH | 24 hr | 3-6 days | 8-14 days |
Microscopic Morphology of MI:
- Necrotic myocardium, acute inflammation ( 1- 3 days after MI ).
- Wave of macrophages that remove necrotic myocardium ( 5- 10 days after MI ).
- Formation of granulation tissue ( 1- 2 weeks after MI).
- Scaring ( most advanced by the end of 6th week ).
Localization of MI:
- Distribution of coronary artery thrombosis;
. Left anterior descending = 45%
. Right coronary artery = 35%
. Left circumflex coronary artery = 15%
- ECG consist of Q waves, ST segment elevation, T- waves inversion.
- Inverted T waves = area of ischemia at the periphery of the infarct.
- Elevated ST segment = injured myocardial cells surrounding the area os necrosis.
- New Q waves = area of coagulation necrosis.
- ECG diagnosis of MI can localized the affect site.
| Area of infarction | ECG changes | Artery involved |
| Inferior wall MI | II, III, a VF | Right coronary |
| Anteroseptal MI | V1-V2 | Left anterior descending |
| Anterolateral MI | V4-V6 | Left circumflex |
| Lateral wall MI | I,ALL, V5, V6 | Left circumflex |
| Posterior | V1-V4, ST segment, upright T waves | Posterior descending |
Complication of MI;
- Arrhythmia
- Third degree heart block;
- Contractile dysfunction.
- Papillary muscle dysfunction.
- Right ventricular infarction.
- Myocardial rupture.
- Chamber dilation.
- Mural thrombus.
- Ventricular Aneurysm.
- Progressive late heart failure.
Leave a Reply